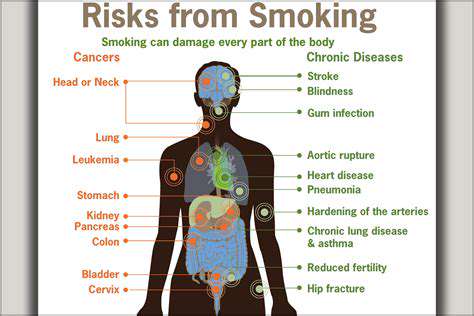
The Impact of Smoking on Circulation in the Legs
Catalog
- Smoking leads to narrowing of the leg arteries, obstructing normal blood flow.
- 20% of smokers under 60 will develop peripheral artery disease (PAD).
- Nicotine causes vasoconstriction, exacerbating circulation problems.
- Long-term smoking may lead to tissue ischemia and severe pain.
- Smokers have three times the risk of developing PAD compared to non-smokers.
- Improvement in leg circulation can occur within two weeks of quitting smoking.
- Pain and numbness in the legs during activity are common warning signs.
- Cold feet indicate inadequate blood supply caused by smoking.
- Smoking significantly increases the risk of thrombosis and vascular lesions.
- Early intervention can prevent severe complications.
- A healthy lifestyle accelerates recovery after quitting smoking.
- Professional guidance can enhance smoking cessation success rates.
- Regular exercise improves cardiorespiratory function after quitting smoking.
- A balanced diet aids vascular repair.
- Personalized smoking cessation plans require medical team support.
How Smoking Harms Blood Circulation in the Lower Limbs
Mechanism of the Lower Limb Circulatory System
The femoral artery and its branches are responsible for delivering oxygenated blood to the lower limbs. Harmful substances in tobacco accelerate endothelial damage, leading to the formation of atherosclerotic plaques. This pathology not only narrows the vascular pathway but also reduces the ability of leg muscles to receive oxygen. Data show that the incidence of peripheral artery disease among smokers is 2-3 times higher than that of the general population.
Even more alarming, when vascular narrowing exceeds 70%, persistent pain may occur even at rest. Clinical observations reveal that about 15% of PAD patients will progress to severe limb ischemia within five years, making limb-salvaging treatments extraordinarily difficult.
Dual Destructive Effects of Nicotine
Nicotine, as a core component of tobacco, has effects that go far beyond addiction. It can trigger systemic vascular spasms within 10 seconds of inhalation, causing foot blood flow to plummet by over 40%. Worse yet, nicotine also stimulates the secretion of adrenaline, leading to spikes in blood pressure and abnormal platelet aggregation.
Research by the British Heart Foundation shows that individuals who smoke 20 cigarettes daily have a dorsalis pedis artery blood flow velocity that is 37% slower than non-smokers. This chronic ischemic state ultimately leads to structural changes in the capillary network, creating a vicious cycle.
Ineversible Vascular Damage Process
Among patients who have smoked continuously for more than ten years, about 65% will exhibit vascular calcification. Such calcium deposits cause arteries to lose elasticity, much like how a rusty pipe cannot expand and contract normally. When the ankle-brachial index (ABI) falls below 0.9, it usually indicates moderate to severe circulatory problems.
Advanced patients often present with characteristic 'smoker's foot'—cyanosis of the toes, skin atrophy, with minor injuries potentially leading to non-healing ulcers. At this point, even if they quit smoking, the established organic changes are difficult to completely reverse.
Typical Manifestations of Smoking-Induced Circulation Disorders in the Lower Limbs
Early Warning Signal Identification
Calf pain during walking is the earliest warning sign, medically referred to as intermittent claudication. This pain follows a typical pattern of 'walking-pain-rest-relief' and is often mistaken for muscle fatigue. As the condition progresses, walking distances can decrease from an initial 500 meters to less than 50 meters.
Another significant signal is tingling in the feet during nighttime sleep. Because the efficiency of the heart in pumping blood decreases while lying down, ischemic symptoms are particularly pronounced at night, leading many patients to dangle their lower limbs to alleviate pain.
Skin Tissue's Distress Signals
Careful observation of changes in lower limb skin can reveal important clues:
• Wax-like sheen on the skin of the feet
• Thickened, deformed toenails that grow slowly
• Unexplained hair loss on the feet
These signs indicate that microcirculation has been severely compromised, making immediate smoking cessation and treatment particularly critical.
Abnormal Temperature Sensation
Patients often complain that their feet feel as if they are 'soaked in ice water,' and this cold sensation is difficult to alleviate even with hot water bottles. Infrared thermal imaging shows that the feet of smokers are generally 2-3°C cooler than those of non-smokers. When the temperature difference between the left and right foot exceeds 2°C, it often indicates severe narrowing of blood vessels on one side.
Long-Term Dangers of Smoking on Lower Limb Vessels
Significantly Increased Amputation Risk
Vascular surgery data indicate that the amputation risk for diabetic smokers is increased by 8 times. Even after successfully quitting for 5 years, their residual risk remains three times higher than that of never smokers. This is because nicotine permanently alters the gene expression of vascular endothelial cells.
A Perfect Breeding Ground for Thrombosis
Carbon monoxide in tobacco smoke reduces hemoglobin's oxygen-carrying capacity by 30%, making blood thick and viscous like porridge. This state particularly facilitates turbulence at the branching points of blood vessels, creating ideal conditions for thrombosis. The incidence of thrombosis above the ankle joint in smokers is 4.7 times that of the general population.
Hidden Microcirculation Crisis
Recent research has found that smoking selectively destroys small blood vessels with diameters less than 200 micrometers. The loss of these vessels does not immediately trigger symptoms but gradually leads to:
• Muscle fibrosis
• Reduced nerve conduction velocity
• Loss of wound healing capability
These changes typically don't become evident until after 10-15 years of smoking.
Scientific Evidence-Based Strategies for Quitting Smoking and Improving Circulation
Timing of Smoking Cessation and Vascular Repair
24 hours after quitting, the levels of carbon monoxide in the blood can return to normal. Within 72 hours, bronchial cilia begin to regenerate, which is crucial for improving overall oxygenation. Clinical data show that quitting smoking for 1 month can increase the microcirculation speed in the toenails by 28%.
The Key Role of Exercise Prescription
It is recommended to adopt a 'intermittent walking training' approach:
1. Walk at a speed that induces mild discomfort
2. Rest until symptoms completely disappear
3. Repeat 5-8 times per day
This training promotes the establishment of collateral circulation, with results superior to medication alone.
Nutrition Support Plan
Vitamin B3 (niacin) can effectively improve endothelial function and is advised to be supplemented through the following foods:
At the same time, intake of trans fatty acids should be limited, as these substances can negate the vascular repair benefits brought by smoking cessation.
Timing for Medical Intervention
When the ankle-brachial index falls below 0.4, mere lifestyle changes are insufficient to improve the condition. At this point, a vascular surgeon needs to assess whether procedures such as:
• Angioplasty
• Plaque excision
• Bypass grafting
are necessary. Early surgical intervention combined with smoking cessation can increase the 5-year limb salvage rate from 40% to 85%.
Read more about The Impact of Smoking on Circulation in the Legs




Hot Recommendations
- The Importance of Hand Care in Scientific Professions
- Exercises to Enhance Balance and Prevent Falls
- The Impact of High Heels on Foot Structure
- Preventing Foot Blisters During Long Walks
- Managing Plantar Fasciitis: Tips and Strategies
- Preventing Foot Injuries in Athletes
- The Benefits of Yoga for Foot Flexibility
- The Relationship Between Obesity and Foot Problems
- The Impact of Flat Feet on Overall Posture
- Addressing Bunions: Causes and Treatment Options